Pustular Psoriasis
Pustular psoriasis presents as fluid-filled pustules which form on top of red or darkened skin.
About pustular psoriasis
‘Pustular psoriasis’ can refer to two different types of psoriasis with similar names: Pustular Psoriasis of the palms and soles (also referred to as palmoplantar pustulosis or acropustulosis), and Generalised Pustular Psoriasis refers to pustular psoriasis across the body.
Palmoplantar Pustulosis (PPP)
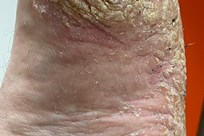
What are the main signs and symptoms of PPP?
The main sign of PPP is patches of very red or dark skin on the palms of the hands or soles of the feet, covered with small pustules. These pustules are filled with fluid which often gives them a yellow or cream colour, and they may dry up and turn brown or crusty after they have burst. The red or darkened skin around the pustules is often thick and flaky, and is often prone to cracking. Because of this, PPP can be painful, and can make walking or using the hands difficult.
As with other types of psoriasis, PPP can be anything from mild to severe, and can wax and wane.
What causes PPP?
The cause of PPP is not completely understood. It is thought to be an autoimmune condition (where the immune system attacks its own body), which appears to particularly affect the eccrine sweat glands; most of which are on the palms and soles. It can occur at any age, but is rare in childhood. PPP can affect either gender, but is more common in women.
Although up to 20% of people with PPP have psoriasis elsewhere on their body, this means that the majority do not. Simply having psoriasis is not thought to trigger PPP.
PPP is more common in women than men, and also in people who smoke or have smoked in the past. Associations with diabetes, arthritis, thyroid disorders and coeliac disease have also been found.
How can PPP be treated?
Topical Treatment
Treatment is likely to begin with topical (applied to the skin) treatments, including steroid creams and coal tar applications. A healthcare professional may advise steroid-based treatments to be applied under occlusion (applied and then wrapped under clingfilm, for instance), as it can help the treatment it to be absorbed through thickened skin. This must only be done on advice from a healthcare professional, and is not appropriate for all types of psoriasis or all body areas.
Other topical treatments such as coal tar or salicylic acid may also be used, to help reduce thick scaling.
As with all types of psoriasis, it is important to moisturise well and regularly, as this will help the skin to feel more comfortable, and can help ‘active’ topical treatments (such as steroid creams) to be better absorbed. In the case of PPP, moisturising can also help to prevent or reduce cracking of the skin.
PUVA
PPP can be stubborn to treat, and, should this be the case, a Dermatologist may prescribe a course of Psoralen Ultraviolet A (PUVA) therapy. PUVA therapy for the hands and feet involves taking oral psoralen or applying topical psoralen to the affected areas before exposure to the ultra-violet A radiation. This is especially useful for the feet as the patient sits with the soles exposed to a small UVA machine, as opposed to standing in a cabinet, where the soles are not reached by light.
Systemic and Biologic Treatments
Other medications that can be used to treat PPP include the oral retinoid acitretin, and oral systemics methotrexate and ciclosporin. Whilst biologic injection treatments are available for the treatment of severe psoriasis, certain types have been found to trigger or worsen PPP, and so these should be avoided.
Generalised Pustular Psoriasis
What is generalised pustular psoriasis?
When pustular psoriasis occurs on areas of the body other than the palms and soles, it is known as ‘Generalised pustular psoriasis’ (GPP) or ‘von Zumbusch pustular psoriasis’. This is different and unrelated to palmoplantar. Again, the fluid in the pustules is not an infection or bacteria, and the pustules are not contagious.
GPP is quite rare, but it is a serious condition that requires urgent medical attention.
What are the main signs and symptoms of GPP?
As with PPP, the main symptom of GPP is small pustules on a background of very red or dark skin, on any area of the body. These pustules are filled with fluid which often gives them a yellow or cream colour, and they often merge into one another to create large areas of pus. These areas eventually dry and peel, before new crops of pustules appear. The skin often feels hot to the touch, and may be sore, tender or itchy.
GPP can spread very rapidly, and can make the person who has it feel quite unwell, due to the skin being overwhelmed and unable to control the body’s temperature. They may have feverish symptoms, such as a headache, nausea, a high temperature, shivering, and feeling hot or cold and tired.
What causes GPP?
The precise cause of GPP is unknown. Some people who develop GPP have, or have previously had, another form of psoriasis, but this is not always the case.
There are a number of potential triggers for GPP, although these are not true to every person, and many people do not identify the trigger for their condition. Possible triggers include:
- Suddenly stopping any kind of steroid medication (steroids should always be weaned off)
- Medications, including certain anti-depressants, certain sedatives or anti-epileptics, certain beta blockers, certain non-steroidal anti-inflammatories, hydroxychloroquine, salicylates, and topical treatments that cause irritation or that are put under occlusion (covered)
- Infections or other illnesses
- Pregnancy
How can GPP be treated?
GPP is a serious condition, so it is essential that medical advice and treatment is sought immediately. People with GPP often need to stay in hospital to get more fluids into the body, stabilise temperature, and try to carefully bring the skin under control.
Treatment for GPP is usually cautious, to hopefully avoid aggravating the skin any further. Initially, affected areas will be treated with bland non-‘active’ treatment, for example emollient, compresses and/or oatmeal baths, to soothe the skin. Treatment may then move onto acitretin - an oral retinoid - or other systemic or biologic medications. PUVA may be used if appropriate. Antibiotics may also be prescribed, if an infection is present.
February 2017 (Review Date: February 2020)